

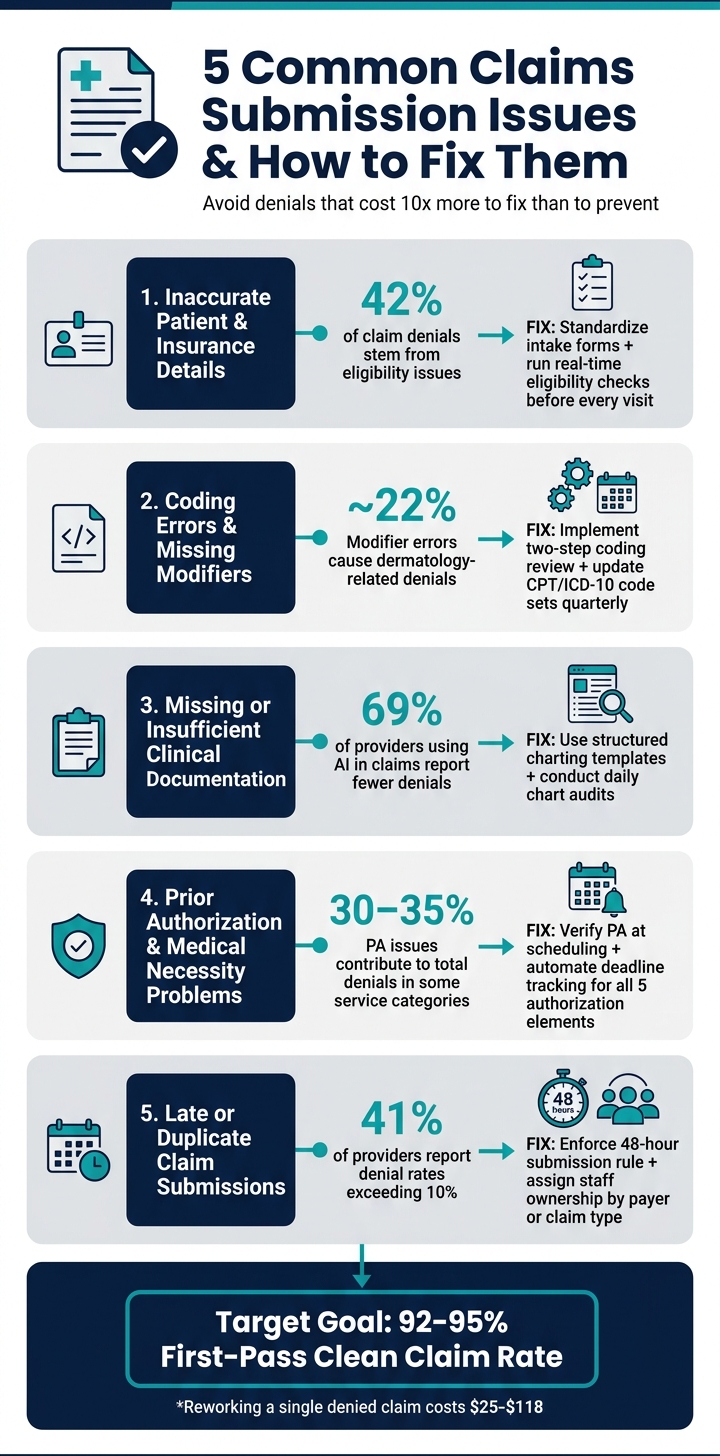
Submitting clean claims is critical for aesthetic and wellness clinics to maintain steady revenue. Yet, many practices struggle with denials, which can cost over 10 times more to fix than filing claims correctly the first time. Here are the five most common claims submission issues and how to solve them:
- Inaccurate Patient/Insurance Details: Typos, outdated insurance info, or missing subscriber data can cause rejections. Fix: Standardize intake forms and verify details at every visit.
- Coding Errors: Incorrect or outdated codes and missing modifiers often lead to denials. Fix: Regularly update code sets and implement a two-step coding review.
- Missing Documentation: Insufficient clinical notes fail to justify medical necessity. Fix: Use structured templates and conduct daily chart audits.
- Prior Authorization Problems: Missing or mismatched authorizations delay claims. Fix: Track authorizations carefully and align billed services with approval details.
- Late or Duplicate Submissions: Filing claims late or multiple times triggers denials. Fix: Assign staff ownership and enforce submission deadlines.
5 Common Claims Submission Issues & Fixes for Clinics
Issue 1: Inaccurate or Incomplete Patient and Insurance Information
Even small data entry mistakes at the front desk can cause major headaches. A typo in a name, a swapped digit in a birthdate, or an outdated insurance ID can result in a claim being rejected before it’s even reviewed. In fact, patient eligibility issues - like inactive coverage or incorrect subscriber IDs - are responsible for nearly 42% of all claim denials.
These errors often stem from common problems like demographic mismatches (misspelled names, wrong birthdates, or gender errors), invalid or expired insurance details, missing subscriber relationship data, and incorrect payer routing codes. The underlying issue? Data that wasn’t properly verified.
"Front-end data accuracy remains one of the most effective levers organizations can pull to reduce downstream denials." - MGMA
The cost of fixing a single denied claim ranges from $25 to $118. Worse, between 50% and 65% of denied claims are never reworked, leading to significant revenue losses. For a busy aesthetics or wellness clinic, even a few of these mistakes each week can add up quickly.
Addressing these errors starts with improving the accuracy of data collected at check-in.
Fix: Standardize Intake Forms and Run Eligibility Checks Before Each Visit
The best way to avoid these issues is to catch errors early - before a claim is created. This begins with a two-step verification process at check-in. Every visit, front-desk staff should compare the patient’s government-issued ID and current insurance card with the system record, not just during initial registration. Given how often insurance details change, it’s also crucial to run real-time eligibility checks (via 270/271 transactions) both when scheduling and again 24–48 hours before the appointment. This allows time to resolve any issues without delaying care or billing.
Systems with mandatory-field validation (or "hard stops") can also prevent incomplete records from being saved. For instance, if a subscriber ID or birthdate is missing, the system won’t allow the entry to proceed, ensuring claims aren’t submitted with blank or placeholder information.
Prospyr offers digital intake forms that include these required-field validations. Its CRM/EMR integration directly streams patient data into billing workflows, reducing the need for error-prone manual data entry.
sbb-itb-02f5876
Issue 2: Coding Errors and Missing Modifiers
Accurate coding is just as crucial as precise patient data when it comes to ensuring smooth claims processing. Even if patient data is spot-on, coding mistakes like incorrect CPT codes, outdated ICD-10 codes, or missing modifiers can still lead to costly denials. These errors are common but avoidable, and they often create unnecessary headaches for clinics.
CPT codes are updated yearly by the AMA, while ICD-10 codes see regular revisions from CMS. Relying on "favorite" codes saved in your system can lead to the use of outdated or invalid options. Additionally, payers are increasingly rejecting "unspecified" ICD-10 codes, demanding the most detailed diagnosis available. If a diagnosis doesn’t logically support a billed procedure - violating Local Coverage Determinations (LCDs) - the claim is flagged for a medical necessity denial. This highlights the need for meticulous attention to coding, just like patient data.
Payers like UHC, Cigna, and Aetna use algorithms to screen claims and may reclassify treatments such as Botox or laser procedures as cosmetic unless the documentation clearly justifies a qualifying diagnosis. Modifiers also play a critical role in avoiding denials related to bundled services.
Modifiers are often a source of revenue loss. Without the correct modifier, payers might assume two procedures are duplicates or bundled together, reimbursing for only one. Modifier errors - especially with Modifier 25, 59, and the X-series - account for about 22% of dermatology-related claim denials. By 2026, Medicare and many commercial payers will favor the more specific X-modifiers (XE, XS, XP, XU) over the broader Modifier 59. For example, using Modifier XS (Separate Structure) when billing for procedures on different anatomic sites can help avoid unbundling denials.
Here’s a quick-reference guide to some commonly used modifiers:
| Modifier | Purpose | What Happens Without It |
|---|---|---|
| Modifier 25 | Separate E/M service on the same day as a procedure | Lost reimbursement for the office visit |
| Modifier 59 / XS | Distinct procedural service at a different site | Payer may only pay for one procedure |
| Modifier 50 | Bilateral procedure | Triggers bundled payment denials |
| Modifier 79 | Unrelated procedure during post-op period | Denied as part of the global surgical package |
Fix: Add Coding Review Steps and Keep Resources Current
The best way to tackle coding errors is by implementing a two-step review process. First, a clinician verifies the diagnosis and procedure details. Then, a trained coder ensures the codes, modifiers, and documentation align before the claim is submitted. This dual review system can catch errors that might slip past a single reviewer, directly protecting your clinic’s revenue. With focused staff training and stronger claim reviews, clinics can reduce denials by 25–30% within 90 days.
To avoid problems with Modifier 25, document the E/M note separately from the procedure note. This ensures clear evidence of distinct medical decision-making. Clinical templates should also be tailored to capture the specific details payers require - like functional impairment, lesion measurements, and complexity levels - so that medical necessity is clear from the documentation itself.
Regular updates are critical. Quarterly audits of CCI (Correct Coding Initiative) edits can help prevent unbundling errors, while frequent reviews of code sets ensure your team stays aligned with the latest AMA and CMS changes. Using a system that pulls real-time, updated codes can significantly lower the risk of submitting outdated information.
Tools like Prospyr offer centralized CRM/EMR integration and AI-powered note creation to help clinicians document the clinical details needed for accurate coding. This reduces the gap between what’s documented and what’s billed, streamlining the entire process.
Issue 3: Missing or Insufficient Clinical Documentation
Even with accurate data and proper coding, claims can still be denied if the clinical documentation doesn't meet payer requirements. This is particularly important in aesthetic and wellness practices, where treatments often blur the line between medical necessity and cosmetic enhancement. Thorough and compliant documentation is essential to avoid denials.
Payers typically require detailed records of what was performed and why the procedure was necessary. For example, treatments like laser therapy for rosacea or Botox for hyperhidrosis must include notes on symptom duration, previous treatments, functional impact, and the rationale for the procedure. A vague note such as "patient requested treatment" won’t cut it. Without a clear and supportive narrative, claims are at risk of being flagged for missing information, leading to delays and added costs.
The root of the problem often lies in fragmented processes. When intake forms, clinical notes, and billing records are managed separately, it’s easy for critical details to fall through the cracks. Without a unified system, no single team member has a full view of the documentation before submitting a claim. As Experian Health highlights:
"Incomplete documentation, coding, and eligibility mistakes rank among the top five most preventable reasons for claims denials."
Disjointed systems not only increase the risk of errors but also make it harder to maintain consistent and accurate records. Closing these gaps requires streamlined and standardized processes.
Fix: Use Standardized Documentation Templates and Daily Chart Audits
To address documentation issues, structured templates and regular audits are game-changers. Standardized charting templates, tailored to meet payer requirements, guide clinicians to document essential details - like symptom duration, prior treatments, clinical rationale, and functional impact. This ensures that critical information is captured every time, leaving no room for guesswork.
Daily chart audits are another effective tool. These audits help catch errors such as missing signatures or incomplete narratives before claims are submitted. Pairing these audits with automated alerts for incomplete fields can significantly reduce manual effort. In fact, 69% of providers using AI in claims management report fewer denials. This shows how technology can simplify the process of validating documentation.
Solutions like Prospyr offer integrated CRM/EMR tools and AI-powered note creation features to enhance consistency. Clinicians can generate structured, real-time notes directly linked to the patient record, ensuring that what happens during the visit is accurately reflected in the documentation. This reduces the risk of errors and helps keep claims moving smoothly through the system.
Issue 4: Prior Authorization and Medical Necessity Problems
Prior authorization (PA) processes continue to be a major hurdle in claims management, especially as they rank among the costliest challenges for healthcare organizations. By 2026, 62% of healthcare organizations identified PA requirements as a leading obstacle. These issues contribute to 30% to 35% of total denials in certain service categories. While efforts to improve data accuracy, coding, and documentation have reduced some denials, tackling PA challenges is now essential for further streamlining claims submission. For aesthetic and wellness clinics, the stakes are particularly high, as many procedures straddle the line between cosmetic and medically necessary.
That distinction is critical for payers. For example, a laser treatment for rosacea or a scar revision might be medically justified, but without clear documentation of functional impairment - such as pain, limited mobility, or failed conservative treatments - payers often classify it as cosmetic and deny the claim outright. The situation is further complicated by the use of AI-driven tools by major insurers like UnitedHealthcare, Cigna, and Aetna. These systems scan claims for specific clinical language, and if the right keywords or measurements are missing, the claims are flagged and denied automatically.
As one expert at ProMBS explained:
"AI-driven denial decisions return results 40% faster than human reviewers, but this speed often comes with increased denials. These automated systems do not evaluate medical necessity the way a physician would." - ProMBS
Denials are also frequently caused by missing authorization numbers, expired approvals, or mismatches between authorized and billed CPT/HCPCS codes. These errors can lead to significant delays, especially as many payers, such as certain Blue Cross Blue Shield plans, have reduced appeal windows from 60 days to just 30 days. In such a tight timeframe, correcting these gaps becomes even more challenging.
Creating a streamlined PA process is crucial to reducing these denials and ensuring claims are approved on the first submission.
Fix: Build a Structured Prior Authorization Process With Deadline Tracking
Preventing PA denials requires treating authorization as a pre-service control rather than a billing task. This means verifying PA requirements at the time of scheduling and reconfirming them during patient check-in. For claims to succeed, every detail must align perfectly with the authorization record, covering these five key elements:
| Authorization Element | Why It Matters |
|---|---|
| CPT/HCPCS Code | Must exactly match the billed service |
| Provider NPI | Authorization often applies to a specific clinician |
| Service Location | Some approvals are site-specific |
| Validity Dates | Services must occur within the approved timeframe |
| Authorized Units | Billed volume cannot exceed approved units |
Manually tracking these elements often leads to mistakes. Automated systems, however, can send alerts when authorizations are about to expire or when approved units are nearly exhausted, significantly improving first-pass approval rates. Clinics that switch from manual to automated PA workflows often see approval rates rise from 75–85% to 90–95%, while the time spent per authorization drops from 25–35 minutes to just 5–10 minutes.
Platforms like Prospyr provide tools to build these structured workflows. Their task management and analytics features allow clinics to assign responsibility for high-volume payer authorizations, track deadlines with automated reminders, and identify bottlenecks through detailed analytics. By addressing these issues proactively, clinics can avoid recurring patterns of PA-related denials and improve overall efficiency.
Issue 5: Late, Duplicate, or Untracked Claim Submissions
Even after overcoming prior authorization (PA) challenges, claim submission timing and duplication can still derail the process. Claims that are filed late or submitted multiple times - even when correctly coded - often face automatic denial. Filing deadlines vary depending on the payer. For example, Medicare gives up to 12 months from the date of service, while most commercial insurers set stricter deadlines, usually between 90 and 180 days. Secondary claims add another layer of complexity, as their submission windows only start after the primary payer's remittance. Missing these deadlines can lead to permanent denials.
The main culprits behind these issues are operational inefficiencies. Manual processes, disconnected systems, and understaffed billing teams can cause claims to stall or even disappear. As Experian Health explains:
"Denial backlogs can quickly become overwhelming, increasing the odds of items slipping through the cracks or missing re-submission and appeals deadlines."
Rejected claims that aren’t addressed promptly are one of the most common reasons deadlines are missed. When these operational gaps go unresolved, they amplify earlier challenges related to coding and documentation.
Duplicate submissions pose another problem. Without a centralized tracking system, duplicate claims often occur, wasting time and triggering denials. With 41% of providers reporting denial rates exceeding 10%, minimizing these errors is critical.
Fix: Set Submission Deadlines and Assign Clear Staff Ownership for Claims
To tackle these challenges, clinics should adopt a structured approach. Start by enforcing a 48-hour submission rule - aim to file all claims within 24–48 hours of the service date. This quick turnaround allows time to identify and fix rejected claims before payer deadlines become an issue. Use a dedicated deadline calendar to track filing windows, coordination of benefits (COB) timelines, and appeal deadlines within your practice management system.
Clear staff accountability is another key step. Over 40% of providers report that assigning specific team members to handle claims significantly reduces denials. Instead of leaving claims tracking to whoever is available, assign staff to specific payers or claim types and hold them responsible for managing aging claims.
Tools like Prospyr's task management and practice analytics platform can help streamline this process. These tools allow clinic managers to assign claim-related tasks, set automated deadline reminders, and monitor claims through a centralized dashboard. Automated status monitoring even provides updates on claim progress weeks before electronic remittance advice (ERA) processing, giving teams the chance to resolve issues before they escalate into denials.
Implementation Checklist for Clinic Managers
This checklist highlights key steps clinic managers can take to reduce claims submission errors, broken down into immediate actions and longer-term strategies.
| Category | Action | Frequency |
|---|---|---|
| Quick Win | Verify patient demographics and subscriber ID against the insurance card at check-in | Every visit |
| Quick Win | Run automated eligibility checks before each appointment | Every visit |
| Quick Win | Check for duplicate claims before resubmitting any rejected claim | Per rejection |
| Quick Win | Use modifier checklists by procedure type (e.g., -25 for E&M with procedures) | Every visit |
| Long-Term | Refresh CPT and ICD-10 code sets and "favorites" lists | Quarterly |
| Long-Term | Audit chart-to-claim documentation templates by visit type | Monthly |
| Long-Term | Review prior authorization status and upcoming deadlines | Daily |
| Long-Term | Assign staff ownership by payer or claim type with clear turnaround times | Ongoing |
By implementing these steps, clinics can drastically improve their claims process. Focusing on front-end accuracy is especially important since registration and eligibility issues alone cause 27% of all claim denials. Plus, reworking a denied claim typically costs over $25.
Assigning clear staff responsibilities also plays a big role in boosting claims accuracy. According to the Revenue Cycle Blog, dividing tasks by expertise is key: patient access teams should manage eligibility rejections, HIM/coding staff should handle medical necessity edits, and billing teams should address format and routing issues.
Aiming for a first-pass clean claim rate of 92% to 95% is a realistic goal for high-performing clinics. This becomes easier when staff accountability is tied to clean-claim performance rather than just submission volume.
Tools like Prospyr can make this process even smoother. Their platform combines scheduling, digital intake forms, task management, and practice analytics into one HIPAA-compliant system. With everything centralized, clinic managers can assign tasks, automate reminders, and track performance - all from a single dashboard. This minimizes manual handoffs, which are often where mistakes occur.
FAQs
What’s the fastest way to raise our clean-claim rate?
The fastest way to boost your clean-claim rate is by adopting automated claims management tools designed to focus on accuracy and prevent errors. By categorizing denied claims - such as those caused by registration mistakes or coding problems - you can spot recurring issues and improve your processes.
Using AI for tasks like coding validation and prior authorization helps catch errors early. This not only reduces denials and the need for rework but also simplifies workflows, leading to more accurate claims.
Which modifiers cause the most denials in aesthetics and wellness?
The two modifiers most frequently causing denials in aesthetics and wellness claims are Modifier 25 and Modifier 59. Misusing these modifiers is responsible for approximately 22% of claim denials. Applying them correctly can play a big role in cutting down errors and boosting the chances of claim approval.
How can we prevent prior auth denials before the visit?
To cut down on prior authorization denials, clinics should take a proactive approach. Start by verifying payer requirements early in the process and confirming whether prior authorization is necessary during scheduling. It's also essential to ensure all documentation is complete and accurate well before the service date.
Utilize tools that can identify services requiring prior authorization, monitor approval statuses, and keep staff informed about payer-specific guidelines. Implementing a structured workflow with clear checkpoints can help secure approvals ahead of patient visits and minimize the risk of denials.

