

Chemical peels are categorized aesthetic procedures involving controlled skin injury to promote exfoliation and collagen regeneration. Their legal classification - cosmetic or medical - depends on depth, agent used, and state regulations. Mislabeling can lead to liability or accusations of practicing medicine without a license. Here's what you need to know:
-
Depth Levels:
- Superficial: Targets the epidermis, often performed by licensed aestheticians.
- Medium: Reaches the dermis, typically handled by dermatologists or surgeons.
- Deep: Requires physician oversight and cardiac monitoring due to systemic risks.
-
Key Terms:
- Frosting: Indicates the endpoint of a peel.
- Defatting: Pre-treatment step ensuring even chemical penetration.
-
Agent Considerations:
- Glycolic Acid: Requires neutralization.
- TCA: Depth controlled by concentration, no neutralization needed.
- Phenol: High systemic risk; requires strict monitoring.
-
Documentation Essentials:
- Use precise terms like "chemexfoliation."
- Digital intake consent forms must outline risks (e.g., scarring, pigmentation changes) and aftercare requirements.
Each procedure (chemical peels, laser resurfacing, microdermabrasion, microneedling) has unique legal and clinical standards. Proper terminology, documentation, and compliance with regulations are critical to avoid legal issues.
Key Legal Definitions and Terms for Chemical Peels
Chemical peels, also known as chemexfoliation or dermapeeling, involve applying a chemical agent to the skin to create a controlled injury. This process promotes healing and stimulates collagen production. DermNet NZ describes it as:
"A chemical peel refers to the application of one or more chemicals to the skin which 'burn' off damaged cells, resurfacing the skin."
The term skin resurfacing is commonly used in medical and legal documents. It refers to removing damaged layers of skin to reveal smoother skin with improved melanin distribution and collagen structure. Including these precise terms in patient records and consent forms is crucial. It communicates to regulators, insurers, and patients that the procedure is a deliberate, medically managed intervention. This standardized terminology ensures consistency and supports compliance with legal and regulatory requirements.
Depth Classifications and Legal Considerations
The depth of a chemical peel significantly impacts its legal and clinical classification. Here's a breakdown:
- Superficial Peels: These target only the epidermis and often use glycolic acid (an AHA), salicylic acid (a BHA), or Jessner's solution. Healing typically takes 3–7 days. Licensed aestheticians or nurses may perform these, depending on state laws.
- Medium-Depth Peels: These reach the papillary dermis and use trichloroacetic acid (TCA) at concentrations of 20–35%. Recovery takes 7–14 days, and these procedures are usually performed by dermatologists or plastic surgeons.
- Deep Peels: Using agents like phenol in the Baker-Gordon formula or croton oil, these penetrate the midreticular dermis. Initial healing takes 14–21 days, and the procedure requires cardiac monitoring due to systemic risks like potential cardiac arrhythmias.
Legal Implications of Agent Selection
The choice of chemical agent carries specific legal and procedural responsibilities:
- Glycolic Acid: Requires neutralization with water or an alkaline solution after application.
- TCA: Acts as a keratocoagulant. Its depth is managed through concentration and technique, and it does not require neutralization.
- Phenol: The most legally complex agent. It is absorbed through the skin and metabolized by the liver and kidneys. Rapid application can lead to toxic systemic effects, including fatal cardiac arrhythmias. To mitigate this risk, procedures must be spaced at 20-minute intervals between facial regions.
Proper documentation of agent selection and procedural protocols is critical to demonstrate adherence to the standard of care.
Additional Key Terms for Documentation
Using specific procedural terms in documentation ensures accuracy and defensibility:
- Frosting: Refers to the whitish discoloration on the skin during a peel, signaling keratin agglutination and serving as the clinical endpoint.
- Defatting: The process of removing skin oils with acetone or alcohol before applying the peel. This step ensures even penetration of the chemical agent and must be documented in pre-procedure notes.
Maintaining consistent language across consent forms, intake documents, and treatment records is essential for minimizing liability. Tools like Prospyr streamline this process by offering digital intake forms and integrated CRM/EMR systems. These platforms help ensure uniform terminology and reduce documentation gaps, which can otherwise increase legal exposure.
sbb-itb-02f5876
1. Chemical Peels
Chemical peels are a medically supervised procedure designed to create a controlled burn on the skin. This process, known as keratolysis and keratocoagulation, helps remove damaged layers of skin and encourages new tissue growth. For legal and medical clarity, terms like chemexfoliation and dermapeeling are often used to emphasize that this is a deliberate and regulated treatment.
The depth of a chemical peel plays a critical role in determining the risks, necessary disclosures, and the qualifications of the practitioner performing the procedure. As Professor Gabriella Fabbrocini, MD, explains:
"The depth of the peel is dictated by a number of factors, including the chemicals applied and their concentration, mode of application, and skin type and its condition."
These depth levels directly influence both the legal and medical aspects of the procedure, as outlined in the table below:
| Peel Depth | Consent and Disclosure Requirements | Practitioner Requirement | Systemic Risk |
|---|---|---|---|
| Superficial | Transient burning, mild exfoliation | Licensed aesthetician or nurse (state-dependent) | Negligible |
| Medium | Prolonged hyperpigmentation risk; caution for Fitzpatrick types IV–VI | Dermatologist or plastic surgeon | Low |
| Deep | Cardiac arrhythmias, permanent hypopigmentation; ECG monitoring needed | Physician with cardiac monitoring capability | High |
Consent forms must specifically address these risks, tailored to the depth of the peel. Two important legal terms should be included in these forms:
- "Risk of demarcation": This refers to the visible line between treated and untreated skin, a common aesthetic and legal issue with deep phenol peels due to their bleaching effect. A standard technique to minimize this risk is feathering the peel at the mandibular border.
- "Post-peel compliance": Patients must be informed that improper aftercare, such as picking at peeling skin or neglecting sun protection for at least six weeks, significantly increases the risk of scarring. Proper documentation of this advice is crucial for legal protection.
2. Laser Resurfacing
Laser resurfacing works differently from chemical peels. While chemical peels rely on acids to break down skin layers through keratolysis, laser resurfacing uses selective photothermolysis. Here, light energy is absorbed by chromophores like water and melanin, then converted into heat to target and destroy specific tissue layers. Because this process involves light energy rather than a chemical reaction, it impacts legal documentation and consent requirements in unique ways. This difference shapes how risks are disclosed and how practitioners approach protocols compared to chemical peels.
Laser resurfacing falls into three main categories: ablative, non-ablative, and fractional. Each approach varies in its depth of treatment and risk profile:
- Ablative lasers, such as CO₂ (10,600 nm) and Er:YAG (2,940 nm), remove both the epidermis and parts of the superficial dermis.
- Non-ablative lasers focus on the dermis while leaving the epidermis intact, which reduces risks significantly.
- Fractional lasers create tiny columns of thermal damage surrounded by untreated tissue, which allows for faster recovery compared to full-field ablation.
Unlike chemical peels, which are categorized by depth of penetration, laser depth is measured in microns per pass. For example, a CO₂ laser removes 20–60 μm per pass, while an Er:YAG laser is more precise, removing just 3–5 μm per pass. The outcome depends on factors like wavelength, pulse duration, and fluence. These measurable parameters play a critical role in procedure documentation and adherence to care standards.
"The goal is to ensure adequate but safe depth of penetration of the laser and delivery of sufficient energy to the targeted tissues while minimizing heat transfer to adjacent structures." - StatPearls
Informed consent for laser resurfacing, often facilitated through a patient portal, must address risks that are specific to this procedure. For instance, ocular injury is a unique concern with lasers, requiring both the patient and provider to wear proper eye protection. Consent forms should also outline risks like ectropion, herpes simplex reactivation (necessitating antiviral medication such as valacyclovir for treatments near the mouth , which can be managed through eRX capabilities), and laser-induced dyspigmentation, especially for individuals with Fitzpatrick skin types IV–VI. Additionally, a recent chemical peel can make ablative laser treatments unsafe, requiring a waiting period of six weeks to six months between procedures.
For non-fractional ablative treatments, practitioners look for the "chamois" (yellow) color of the wound bed as a visible endpoint, indicating that the papillary dermis has been reached. Going beyond this point increases the risk of permanent scarring and must be carefully documented. The next section will compare these risks with those of other popular aesthetic treatments.
3. Microdermabrasion
Microdermabrasion stands apart from treatments like chemical peels and laser resurfacing by relying on mechanical exfoliation, which influences both its legal classification and risk profile. This procedure uses either abrasive crystals or a diamond-encrusted wand to physically remove the stratum corneum, the skin's outermost layer, while suction clears away the loosened skin cells. This approach makes it a "minimally invasive epidermal resurfacing procedure", as defined in clinical and legal contexts. Its limited depth of effect is key to its classification and application.
The depth of treatment is critical in defining its legal status. While standard microdermabrasion focuses solely on the stratum corneum, superficial chemical peels can penetrate about 60 μm into the skin, and medium-depth peels go as deep as 450 μm. For instance, Michigan Public Act No. 159 of 2024 mandates physician supervision for any microdermabrasion procedure that goes deeper than the stratum corneum. This means the legal status of a session can change based solely on how deeply the treatment affects the skin.
"I always tell my patients that microdermabrasion is excellent for maintenance and mild concerns, but it's not a transformative procedure." - Dr. Emmy Graber, President, Dermatology Institute of Boston
Informed consent plays a significant role in this process. While microdermabrasion has a lower risk profile than deeper treatments, practitioners must still disclose potential side effects like temporary redness, swelling, skin flaking, and petechiae (small bruise-like spots caused by excessive vacuum pressure). Patients should also be advised to use broad-spectrum sunscreen for at least a week following the procedure, as the skin becomes more sensitive to sunlight. Additionally, the treatment temporarily disrupts the skin barrier, increasing the absorption of topical medications by up to 50%.
Practitioners are legally required to screen for contraindications and document cases where the procedure is unsuitable. Microdermabrasion is not recommended for individuals with active herpes simplex virus (HSV), rosacea, eczema, active inflammatory acne, a history of keloid scarring, or recent isotretinoin use. Consent forms should also instruct patients to report any bleeding, blistering, or swelling lasting beyond 48 hours. It’s important to differentiate microdermabrasion from dermabrasion, a surgical technique that removes deeper layers of skin, involves expected bleeding, and carries a higher risk profile. Understanding these distinctions ensures practitioners stay compliant and provide safe, effective care across various resurfacing methods.
4. Microneedling
Microneedling stands apart from the other treatments mentioned in this article. Instead of relying on chemical agents, crystals, or light, it uses mechanical action - thin needles create controlled punctures in the skin, activating the body’s natural wound-healing process. This, in turn, stimulates the production of collagen and elastin. Because of its unique mechanism, microneedling falls under a different set of regulations compared to chemical or laser-based treatments.
According to the FDA, a microneedling device is defined as one that uses needles to puncture the skin mechanically for aesthetic purposes, as outlined in 21 CFR 878.4430. Motorized microneedling devices designed to alter tissue structure or function beneath the skin are classified as Class II medical devices and are approved for use on patients aged 22 and older. However, devices intended to deliver drugs, cosmetics, or biologics through the skin are not included in this classification.
The depth of the needles is a key factor in determining whether a microneedling procedure is considered cosmetic or medical. For needle depths ranging between 0.25 mm and 0.5 mm, the procedure is generally categorized as cosmetic. When the needle depth exceeds 0.5 mm and reaches into the dermis (up to 2.5 mm or more), it triggers a more extensive wound-healing response, classifying the procedure as medical-grade. In states like California, Florida, and New York, microneedling at dermal depths is officially recognized as a medical procedure, which means it falls outside the scope of a standard esthetician license. This distinction between cosmetic and medical procedures is central to both regulatory guidelines and informed consent.
"The question is not simply 'is microneedling cosmetic or medical?' - it is more nuanced than that. The central variable is needle depth." - MyExosthetics
Because of these classifications, detailed risk disclosures are crucial. Common side effects of microneedling include bleeding, bruising, redness, itching, and peeling. Less frequent risks, such as infections, herpes simplex flare-ups, granulomatous reactions, and scarring, must also be disclosed. For RF microneedling - devices that combine needles with radiofrequency energy - additional risks like burns, fat loss, and nerve damage should be addressed. After the procedure, patients should avoid retinol, glycolic acid, and alcohol-based products, and ensure proper sun protection to safeguard their skin during recovery.
Pros and Cons by Procedure
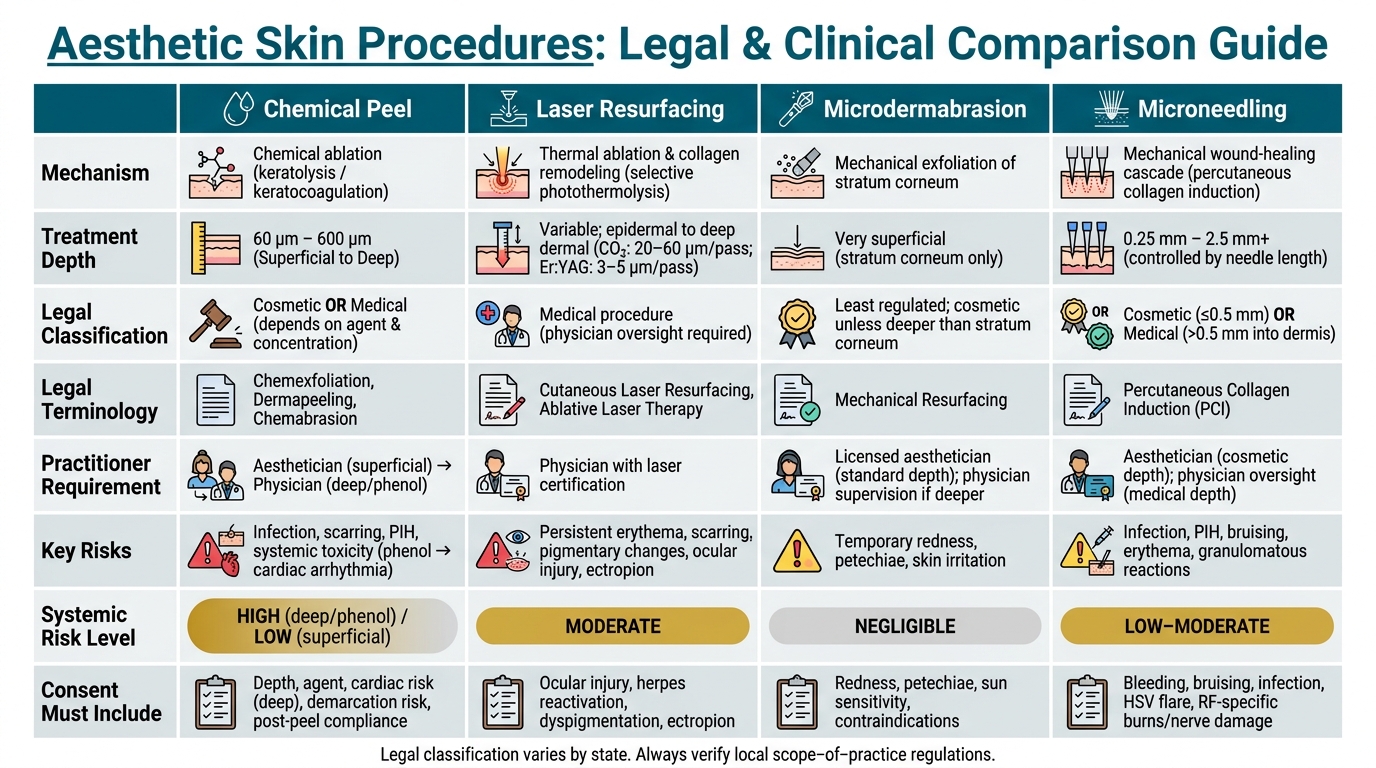
Aesthetic Skin Procedures: Legal & Clinical Comparison Guide
Each procedure varies in its approach, depth of treatment, legal considerations, and associated risks. Understanding these differences is crucial - not just for clinical outcomes but also for proper documentation, consent protocols, and scope-of-practice decisions.
Chemical peels are highly adaptable, offering a range of depths. However, this flexibility also introduces legal complexity. Depending on the agent and concentration, a chemical peel could be a simple cosmetic service or a medical procedure requiring cardiac monitoring. Laser resurfacing operates across a similar depth spectrum but uses thermal energy, which alters its risk profile and documentation needs. Microdermabrasion, on the other hand, is limited to the stratum corneum, making it the simplest option from a regulatory perspective. Lastly, microneedling is unique in its mechanical approach, with needle depth determining its classification and regulatory requirements.
Here’s a breakdown of these procedures:
| Procedure | Mechanism | Depth | Legal Terminology | Key Risks |
|---|---|---|---|---|
| Chemical Peel | Chemical ablation (keratolysis/keratocoagulation) | 60 μm–600 μm (Superficial to Deep) | Chemexfoliation, Chemopeel, Chemabrasion | Infection, scarring, PIH, systemic toxicity (phenol) |
| Laser Resurfacing | Thermal ablation & collagen remodeling | Variable; epidermal to deep dermal | Cutaneous Laser Resurfacing, Ablative Laser Therapy | Persistent erythema, scarring, pigmentary changes |
| Microdermabrasion | Mechanical exfoliation of stratum corneum | Very superficial (stratum corneum only) | Mechanical Resurfacing | Skin irritation, localized redness; avoid 3–4 weeks before peels |
| Microneedling | Physical induction of wound-healing cascade | Variable; controlled by needle length | Percutaneous Collagen Induction (PCI) | Infection, PIH, bruising, erythema |
These distinctions highlight the unique clinical and legal aspects of each treatment.
For example, higher concentrations of AHAs (alpha hydroxy acids) and salicylic acid elevate a peel from cosmetic to medical status, impacting who can administer the procedure and the necessary consent documentation.
"Chemical peels consist of the application of one or more chemical ablative agents to the skin's surface in order to induce keratolysis or keratocoagulation." - Alicia A. O'Connor, Department of Dermatology, Royal Prince Alfred Hospital
Phenol-based deep peels, in particular, demand rigorous consent protocols, including ECG monitoring. At the other end of the spectrum, microdermabrasion has minimal downtime, with risks limited to temporary redness and irritation. Regardless of the procedure, tools like the Fitzpatrick skin phototype scale and the Glogau photoaging classification are essential for documenting baseline skin conditions and are considered standard practice for both clinical and legal purposes.
Conclusion
Legal terminology plays a key role in defining practitioner qualifications, documentation requirements, and liability risks. These distinctions have tangible effects on consent processes and recordkeeping.
Each procedure falls into a specific regulatory category. Microdermabrasion is the least regulated, while chemical peels straddle cosmetic and medical classifications depending on factors like AHA concentration and pH levels. Meanwhile, microneedling and laser resurfacing are considered medical procedures under current regulations, requiring physician oversight and written supervisory protocols.
The choice of terms like "chemexfoliation" versus "chemical peel" in documentation, or properly classifying a peel's depth, significantly impacts risk evaluation and scope-of-practice decisions. Every record must clearly outline the procedure, associated risks, and practitioner responsibilities. As noted by O'Connor et al.:
"A detailed consent discussion should be undertaken by the treating clinician and appropriately documented in the medical record."
From a compliance perspective, practices should retain practitioner records for at least 5 years, display the delegating physician’s name and scope of delegated procedures in the treatment area, and ensure consent forms explicitly describe the procedure, its risks, and confirm that patient questions were addressed.
To reduce risks tied to manual documentation errors, Prospyr simplifies digital recordkeeping. With HIPAA-compliant tools like digital intake forms, CRM/EMR integration, and AI-assisted note creation, it helps practices keep clinical records audit-ready for all types of procedures.
FAQs
When does a chemical peel become a medical procedure?
A chemical peel qualifies as a medical procedure when conducted under the supervision of a physician skilled in skin anatomy and wound healing. The physician assesses its appropriateness by following established therapeutic guidelines.
What should be documented to minimize legal risk for peels?
To reduce legal risks associated with chemical peels, it's crucial for practitioners to maintain thorough documentation. This includes recording the patient's medical history, detailed treatment notes, signed informed consent forms, and pre- and post-treatment care instructions. Additionally, ensure all records are securely stored and kept for the legally mandated period. Accurate and organized documentation safeguards both the patient and the provider.
How do scope-of-practice rules differ for peels vs. microneedling?
Scope-of-practice rules for chemical peels and microneedling can differ based on factors like treatment depth, required supervision, and licensing.
For chemical peels, non-physicians are often allowed to perform superficial treatments, but they must adhere to strict limits on acid concentration and pH levels. For instance, some states permit the use of alpha hydroxy acids (AHAs) up to 30%.
Microneedling, on the other hand, generally demands a higher level of oversight. Licensed practitioners or those working under physician supervision are typically required, especially for procedures involving deeper skin penetration. The regulations become more stringent as the invasiveness of the procedure increases, emphasizing the importance of proper training and safety.

