

If I hire an RN for a California med spa, I can’t treat it like a simple staffing step. I need a file that shows the RN has a current California license, a clear scope tied to written standardized procedures, training records for each service, malpractice coverage that matches the work, and signed policy acknowledgments before any patient care starts.
Here’s the short version:
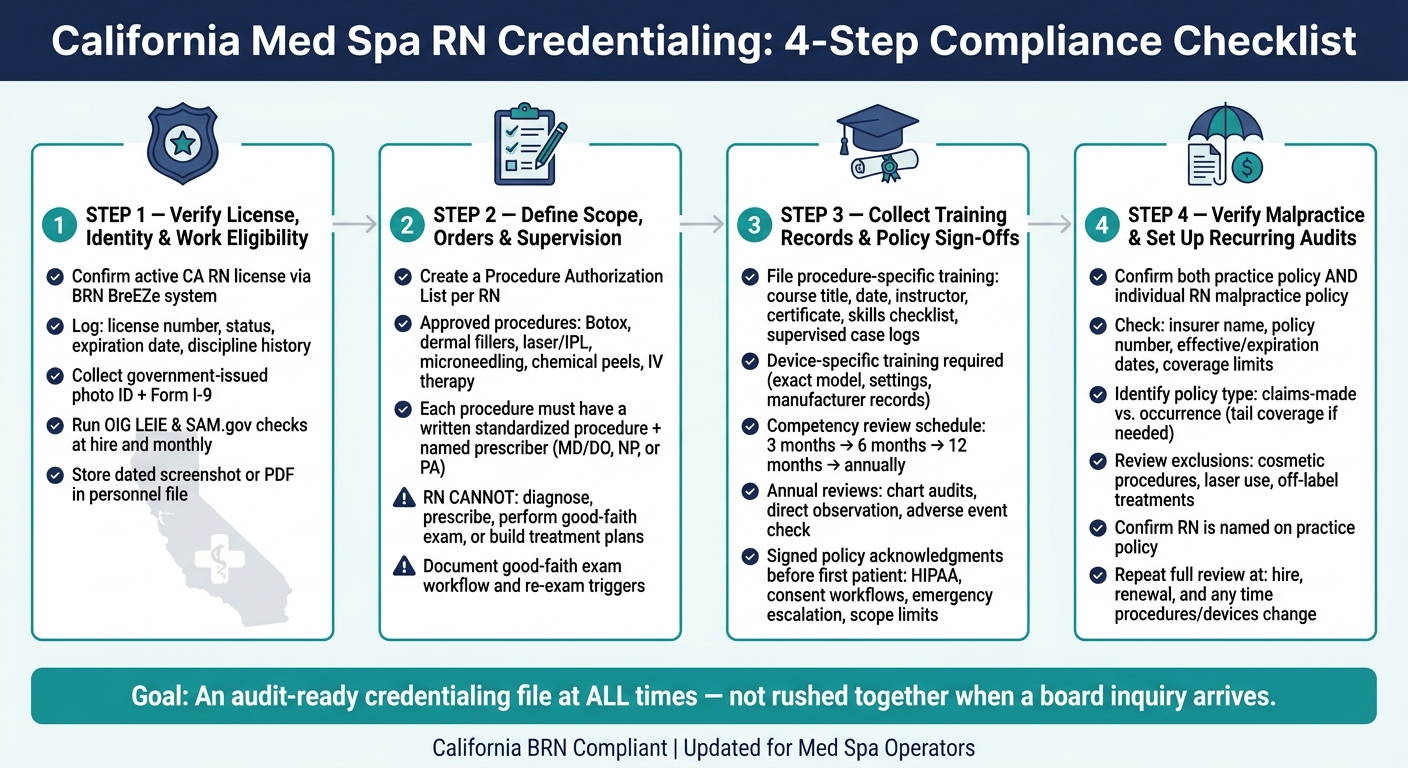
- License first: I verify the RN’s California license, public discipline history, identity, and work eligibility.
- Scope next: I match each service - like Botox, fillers, laser/IPL, microneedling, peels, or IV therapy - to written orders, supervision, and standardized procedures.
- Training by procedure: I keep proof of service-specific training, device training, supervised case logs, and review dates.
- Coverage check: I confirm both practice and individual malpractice policies, including policy type, dates, limits, and exclusions for cosmetic services.
- Audit-ready records: I store dated screenshots, signed policies, and renewal reminders so the file is ready at hire, renewal, and when duties change.
A few points matter most:
- In California, injectables and laser-based cosmetic treatments are medical procedures.
- An RN cannot diagnose, prescribe, do the good-faith exam, or build the treatment plan alone.
- The file should show who examined the patient, who ordered treatment, and who supervises the RN.
- Reviews should happen at set points like 3, 6, and 12 months, then yearly after that.
| Area | What I need on file | Why it matters |
|---|---|---|
| License & identity | Active CA RN license, discipline check, photo ID, I-9 | Confirms the RN can work and practice |
| Scope & supervision | Approved procedure list, written standardized procedures, named prescriber | Shows what the RN may do and under whose oversight |
| Training & review | Course records, device training, case logs, review sign-offs | Shows the RN was trained for each service |
| Insurance | Practice policy, individual RN policy, exclusions, renewal dates | Checks whether claims tied to cosmetic care may be covered |
| Policies & records | Signed acknowledgments, HIPAA/privacy, emergency steps, record storage | Keeps the file complete and easy to review |
Bottom line: if I want to cut compliance and patient-safety risk, I need a repeatable credentialing process - not a stack of last-minute paperwork. The article below walks through that process in the order I’d use it.
California Med Spa RN Credentialing Process: 4-Step Compliance Checklist
Step 1: Verify RN License, Identity, and Work Eligibility
Before an RN performs injectables, laser/IPL, or other aesthetic procedures, make sure three things are checked first: a current California RN license, matched identity, and legal work authorization.
Confirm Active California RN License and Discipline History
Begin with the California Department of Consumer Affairs (DCA) License Search through the BRN's BreEZe system. Use the license number when possible. That helps avoid mix-ups from similar names.
After you open the record, log the following in the credentialing file.
| Field to Record | Why It Matters |
|---|---|
| License number | Main identifier for future re-checks |
| License status (active, inactive, delinquent, restricted) | Confirms the RN is currently allowed to practice |
| Expiration/renewal date | Shows when re-verification is due |
| License class and any public restrictions | Confirms scope of qualification |
| Discipline link reviewed (yes/no) | Shows whether a public discipline document was present |
| Date checked and reviewer initials | Creates a dated record |
Review any probation, reprimand, or surrender record before hire. If you find any restriction, send it to the medical director for written review before onboarding.
No RN should be assigned clinical duties until a current California RN license has been verified and a dated screenshot or PDF printout is stored in the personnel file.
Collect Core Hiring Documents and Background Checks
Verify identity at the same time you verify the license. Collect a government-issued photo ID and make sure the name matches the license record. If the names don’t line up - for example, after a legal name change - keep the supporting paperwork in the file.
Complete Form I-9 within the federal deadline. Review the accepted List A, B, or C documents, record the verification date, and store the form in a secure HR file separate from the clinical credentialing folder.
For background screening, use a provider that knows California's Fair Chance Act and its notice rules, which generally apply to public and private employers with five or more employees. Use a California-compliant criminal-history screening process, and follow Fair Chance Act notice rules before taking adverse action. Run OIG LEIE and, if your program uses it, SAM.gov checks at hire and monthly.
Document Education and Baseline Credentials
Collect proof that the RN completed an accredited nursing program. Record the school name, the accreditation body, such as CCNE or ACEN, and the graduation date. A copy of the diploma or degree certificate gives you a clean baseline record.
| Document | Details to Record |
|---|---|
| Nursing diploma or degree certificate | School name, accreditation, graduation date |
| NCLEX-RN passage | Confirmed via active BRN license |
| Initial licensure date | From BRN license record |
Once license, identity, and work authorization are verified, move to scope of practice and supervision.
sbb-itb-02f5876
Step 2: Match the RN's Role to California Scope, Orders, and Supervision
After license verification, the next step is simple: define exactly what the RN can do, who approves it, and how supervision works.
A California RN license by itself does not give the RN permission to perform aesthetic procedures. Before the first patient visit, you need written records that lay out the RN's scope, supervision setup, and treatment-order path.
List Approved Procedures the RN May Perform
Create a Procedure Authorization List for each RN and store it in the credentialing file. This list should name every aesthetic procedure the RN is allowed to perform, then connect each one to the conditions that must be met before the RN can do it.
That usually includes services like injectables, laser/IPL, microneedling, chemical peels, and IV therapy.
| Procedure | RN Permitted Role | Who Must Order |
|---|---|---|
| Neuromodulators (e.g., Botox) | Administer per signed order | MD/DO, NP, or PA |
| Dermal fillers | Administer per signed order | MD/DO, NP, or PA |
| Laser hair removal | Operate device per protocol | MD/DO, NP, or PA |
| IPL photofacial | Operate device per protocol | MD/DO, NP, or PA |
| Microneedling | Perform per signed order | MD/DO, NP, or PA |
| Medical-grade chemical peel | Perform per signed order | MD/DO, NP, or PA |
The scope summary should also spell out what the RN cannot do. In California, that means the RN may not diagnose, create a treatment plan, prescribe, or perform good-faith exams.
From there, connect each approved procedure to written standardized procedures and to a named prescriber who provides oversight.
Review Standardized Procedures and Prescriber Oversight
Standardized procedures are the legal basis for RN delegation. If this part is fuzzy, the whole setup starts to wobble.
Each standardized procedure should clearly describe:
- The treatments covered
- The patient populations involved
- Any device settings or treatment parameters that apply
- The RN's step-by-step role
- The supervision level required
- The rules for escalation
Each protocol should be written, dated, signed, and listed in the RN's credentialing file.
Prescriber oversight also needs to be tied to a specific person by name. The credentialing file should identify the MD/DO, NP, or PA responsible for oversight and explain how that supervision happens, what the prescriber reviews, and how adverse events are recorded. Many practices use digital intake forms to capture this data efficiently.
A paper-only medical director setup is noncompliant.
Confirm Good-Faith Exam and Treatment-Order Requirements
The credentialing file should include a written policy stating that every patient gets a good-faith exam from a qualified prescriber before initial treatment. The RN does not perform this step under any circumstances.
That policy should also walk through the workflow in plain terms: how the prescriber exam is scheduled online, how the treatment plan is recorded, and when the RN may begin care.
For Botox, require a patient-specific signed order after the good-faith exam has been documented. The file should also note re-exam triggers. For example, if the patient asks for a new indication, the dose changes in a material way, or a set period has passed since the last exam, the prescriber must evaluate the patient again before the RN moves forward.
Step 3: Collect Training Records, Competency Validation, and Policy Sign-Off
Once the scope is set, the next job is to document training and competency for every service the RN will perform.
This is where many clinics get sloppy. A license and approval under standardized procedures are not enough on their own. You need records tied to each procedure, device, and protocol. Under California rules, those records help show the RN is allowed to perform that service. A course completion by itself only shows attendance, not full procedure-level competency.
File Procedure-Specific Training and Device Certificates
For each service the RN may provide, the credentialing file should include:
- Course title
- Training date
- Instructor or training organization
- Certificate of completion
- Skills checklist
- Any supervised case logs
If the service involves a device, get even more specific. File the exact device model, the settings or parameters covered in training, and any manufacturer training records. Generic laser safety training doesn't show competency on one specific platform.
| Procedure | Training Evidence to File |
|---|---|
| Neuromodulators (e.g., Botox) | Injection lab, anatomy review, complication management, supervised case log |
| Dermal fillers | Injection technique course, complication management training, supervised cases |
| Laser / IPL | Device-specific manufacturer training, laser safety education, eye protection protocol |
| Microneedling | Product education, contraindication screening, depth or concentration limits, post-care training |
| Chemical peel | Peel agent training, skin assessment, neutralization protocol, aftercare instruction |
Document Initial and Ongoing Competency Reviews
California standardized procedures call for written initial and ongoing competency evaluation.
Before an RN works on any service without direct supervision, require a formal competency sign-off. That sign-off should name the evaluator, list the tasks observed, record the number of supervised cases completed well, and confirm the RN showed both technical skill and proper follow-through with clinic policy. Direct observation is the preferred way to handle the first assessment because the evaluator can see performance and protocol use as it happens.
Use scheduled reviews at 3, 6, and 12 months, then once a year after that. Each review should connect back to the approved procedure list from Step 2. Put simply, if Step 2 defines what the RN may do, competency review is what checks that the RN can do it the right way.
Annual reviews should include chart audits, direct observation, and a check for any adverse events or complaints since the last review. If an RN rarely performs a certain procedure, don't wait for the annual review to deal with it. More supervision or a refresher makes more sense.
If a gap shows up, start a remediation workflow right away. Document the missing skill, assign retraining, require supervised practice, set a re-evaluation deadline, and note any temporary limits on that procedure while competency is being restored. That gives you a clear paper trail instead of a vague "we handled it."
Get Policy Acknowledgments and Store Records in One Place
Before the RN sees a patient, have them sign every policy acknowledgment. That should cover informed consent workflows, documentation standards, adverse event escalation steps, HIPAA and privacy rules, photography and social media use, infection control, emergency response, and scope-of-practice limits.
Each acknowledgment should be dated, version-controlled, and tied to the policy manual version in effect at that time. If a policy changes later, you don't want any confusion about which version applied.
When records are spread across email threads, paper folders, and different manager files, audits get messy fast. Things slip through the cracks. A HIPAA-compliant platform like Prospyr can keep licenses, training records, reminders, and policy acknowledgments in one place.
Once those training records and acknowledgments are on file, the next step is to confirm malpractice coverage and keep the credentialing file ready for review.
Step 4: Review Malpractice Coverage and Set Up a Recurring Audit Process
Malpractice coverage is a major checkpoint before an RN sees patients. A license and signed policies don't protect the practice if the insurance doesn't actually cover the services the RN is performing.
Verify Individual and Practice Malpractice Coverage
Keep both the practice's malpractice policy and the individual RN's malpractice policy active before patient care starts. Claims often name everyone involved, so both policies need to be in place before the RN begins seeing patients.
For each policy, confirm:
- Insurer name
- Policy number
- Effective and expiration dates
- Coverage limits
Then check whether the policy is claims-made or occurrence. A claims-made policy usually covers claims only while the policy is active, which means an RN who leaves may need extended reporting coverage, often called tail coverage, to avoid a gap. An occurrence policy is tied to when the incident happened, so coverage may still apply after the policy ends.
Read the exclusions closely. Some policies leave out cosmetic or elective procedures, laser use, off-label treatments, or services performed by nonphysician providers. Make sure the policy covers each cosmetic service the RN will perform.
You should also confirm that the RN is listed by name and role on the practice's policy. If a provider is doing procedures but isn't listed, the carrier may deny coverage for any claim tied to that provider.
Log these policy details in the same file you use for license and competency tracking.
Use Tables to Track Scope, Training, and Coverage
Use one coverage audit table to track policy type, exclusions, named providers, and renewal dates. The table should flag insurance gaps, not repeat scope or training records already stored somewhere else.
Coverage documents on file:
| Coverage Type | Document to Keep on File |
|---|---|
| Facility general and professional liability | Declarations page, certificate of insurance, renewal notices |
| Medical director coverage | Applicable policy documents tied to practice structure |
| Individual RN malpractice | Policy declarations, endorsements, extended reporting/tail coverage documents (if applicable) |
Conclusion: Turn the Checklist Into a Repeatable Credentialing Process
Treat malpractice review as a recurring audit item, not a one-time hiring task. Assign one person to own the process. Use a standard checklist, set renewal reminders for licenses and insurance policies, and document corrective actions whenever a file is incomplete.
Run the same review at hire, renewal, and any time procedures change. If procedures, devices, or staffing change, update the credentialing file before the RN performs the new service. A HIPAA-compliant platform like Prospyr can help centralize licenses, training records, insurance documents, and renewal reminders in one place, so nothing slips through the cracks between audit cycles.
The goal is an audit-ready file at all times, not one that's rushed together when a board inquiry or insurance review shows up.
FAQs
Can an RN do Botox alone in California?
No. In California, an RN can give Botox only when a physician has delegated the task, is supervising it, and there is a formal written delegation agreement in place. The RN also has to stay within the legal scope of RN practice.
There’s another limit here: an RN cannot do the required Good Faith Exam. That exam must be done by a physician, nurse practitioner, or physician assistant.
What documents should I collect before an RN starts?
Before an RN starts their first shift, you need a complete personnel file on hand and fully checked. That file should include:
- A current, unrestricted California RN license
- CPR/BLS certification
- DEA registration, if applicable
- Professional liability insurance
- OSHA and HIPAA training records
- Clinical competency and device-specific training documentation
You should also keep a signed, physician-approved SOP that spells out scope of practice and delegation protocols.
And one more thing: don’t rely only on copies sent by the candidate. Verify credentials through official California Board of Registered Nursing lookup tools.
How often should I recheck RN credentials and training?
Recheck each nurse’s license during every renewal cycle through the right state board. At the same time, track expiration dates and continuing education needs all year.
A digital system can make this much easier. Set reminders for 90, 60, and 30 days before each deadline so nothing slips through the cracks. Annual safety and compliance training should stay up to date too, including OSHA Bloodborne Pathogens and HIPAA privacy modules.
